Ever notice how sleep professionals like to talk about sleep hygiene? For those of you who aren’t well read on the literature and science of trying to get to sleep — and I do mean trying — sleep hygiene is the art of making your bedroom the perfect place to sleep. You make it as dark as you possibly can, preferably dark enough to develop your 35 mm film in (for those of you who are old enough to remember that cameras have not always been digital and didn’t come as an afterthought on an iPhone). They also want you to remove all evidence of time. No clocks, even soundless, lightless digital ones. And, oh horrors! Absolutely no real-world ticking clocks. No sound whatsoever, and as much like a recording studio with padded acoustic walls etc., etc. And it must be the perfect sleep temperature, not too hot or too cold. The Goldilocks temperature, one might say. And the firmness of your mattress… Well, you get the idea. Haven’t these people ever heard of deafferentation?
Actually, I wasn’t telling you the truth, not all of it at least, when I said that sleep hygiene was “the art of making your bedroom the perfect place to sleep.” They also want to make you the perfect sleep generator. You must not eat anything too close to bedtime, it might upset your stomach, or too far from bedtime, you might get hungry. (Makes me wonder how many times they were read Goldilocks and the Three Bears as a child.) Caffeine and alcohol are strictly forbidden, and oh yes, you can’t so much as catch a glimpse of a computer screen, or you are condemned to a lifetime of insomnia. Oh, get plenty of sunlight. And workout like a fiend.
It doesn’t stop there. You cannot ever think a bad thought about your bedroom. It must be your perfect haven but only for sleep. Well, you are allowed to have sex there, but not when you should be sleeping, because you must go to sleep at the same time each night and wake at the same time each morning. The worse thing of all is to have a bad attitude toward the amount and quality of sleep you got the previous night, or for that matter, the way you have been sleeping for the last couple of years, or, possibly, decades. No bad thoughts about sleep.
And last of all — and this is when they actually come close to the real problem — they want you to only have pleasant thoughts running through your head while you are trying to go to sleep. No thoughts about that colleague you plan to shove down the elevator shaft the first thing when you get to work in the morning, or perhaps the fact that you are considering getting a cage to lock up your 15 year old. And if the neighbor’s dog doesn’t quit barking you are going to go after both him and the dog with a baseball bat, right now. You can’t think that. Be calm, be nice, be gentle and go to sleep.
Okay. Possibly you can’t get to this sleep state by reading the rules of sleep hygiene off a website, but they have a course you can take, costs only a few hundred dollars, but the really effective way to take it is in residence, which only costs a few thousand. Did I mention that they also have medication? Not quite the same as sleep, but will certainly make you unconscious.
All this is what sleep professionals like to tell insomniacs because they know nothing about getting to sleep. Did you notice that? When you close your eyes, you are on your own. They know nothing about actually getting to sleep. You have thoughts coursing through you brain instead of sleeping? Try meditation. The purpose of meditation is to purge your mind of thoughts and put you in a perfect spiritual state. Perhaps you’ll even talk to God. Well, count sheep then. Count backwards from a thousand. Imagine shooting a hundred free-throws.
But the barking dog. The fifteen year old. And the elevator shaft.
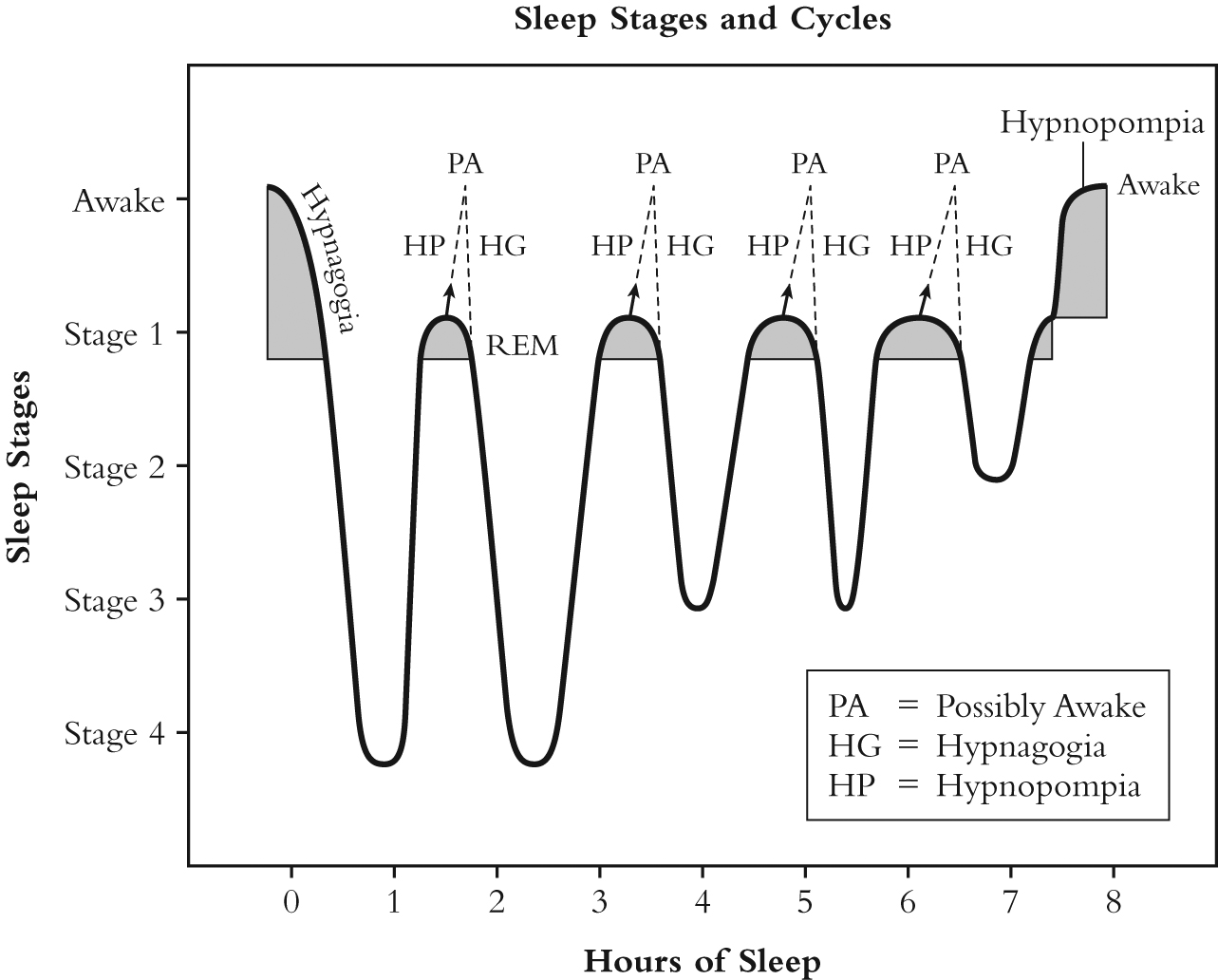
Truth be known, sleep professionals know nothing about actually getting to sleep. Well, maybe that isn’t quite true. Researchers have studied sleep onset, the period of time from when you close your eyes until you are actually asleep. This transition state is also called hypnagogia. We have literature on it going all the way back to Aristotle. A woman, R. E. Leaning, wrote an excellent article on hypnagogia in 1925 titled, “An Introductory Study on Hypnagogic Phenomena.” Daniel L. Schacter wrote an excellent article in 1976 titled, “The Hypnagogic State: A Critical Review of the Literature.” And to top it all off, Andreas Mavromatis has written an excellent book titled, Hypnagogia, The Unique State of Consciousness Between Wakefulness and Sleep. Researchers have also written a book that documents some of their more recent work on sleep onset titled interestingly enough, Sleep Onset: Normal and Abnormal Processes, edited by Robert D. Ogilvie and John R. Harsh, 1994. Ever see any of this literature referenced by any of these so-called sleep professionals? No one. Ever. Mentions. Any of it. Ever.
A cynical person might think that these sleep professionals are making a lot of money off insomniacs and really aren’t interested in solving the problem. A cynical person might think that sleep professionals, therapists, pharmaceutical companies, and charlatans in general have a vested interest in keeping this information from insomniacs because someone might come to understand the true nature of the problem and solve it themselves, without spending a lot of money on online courses, webinars, seminars, retreats, and yes, yes, yes, office visits and medication, medication, medication. Companies could go bankrupt. That someone might write a book. It would destroy the economy, global economy. But let’s not think those cynical thoughts because we could lie awake at night planning to do harm to these people. It could cause insomnia.
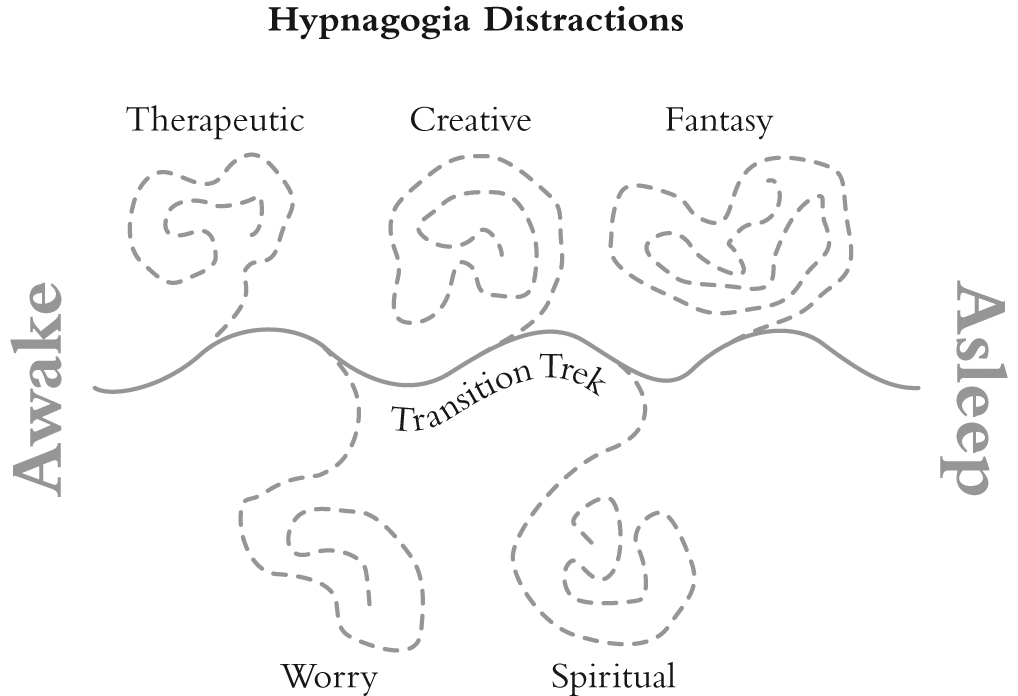
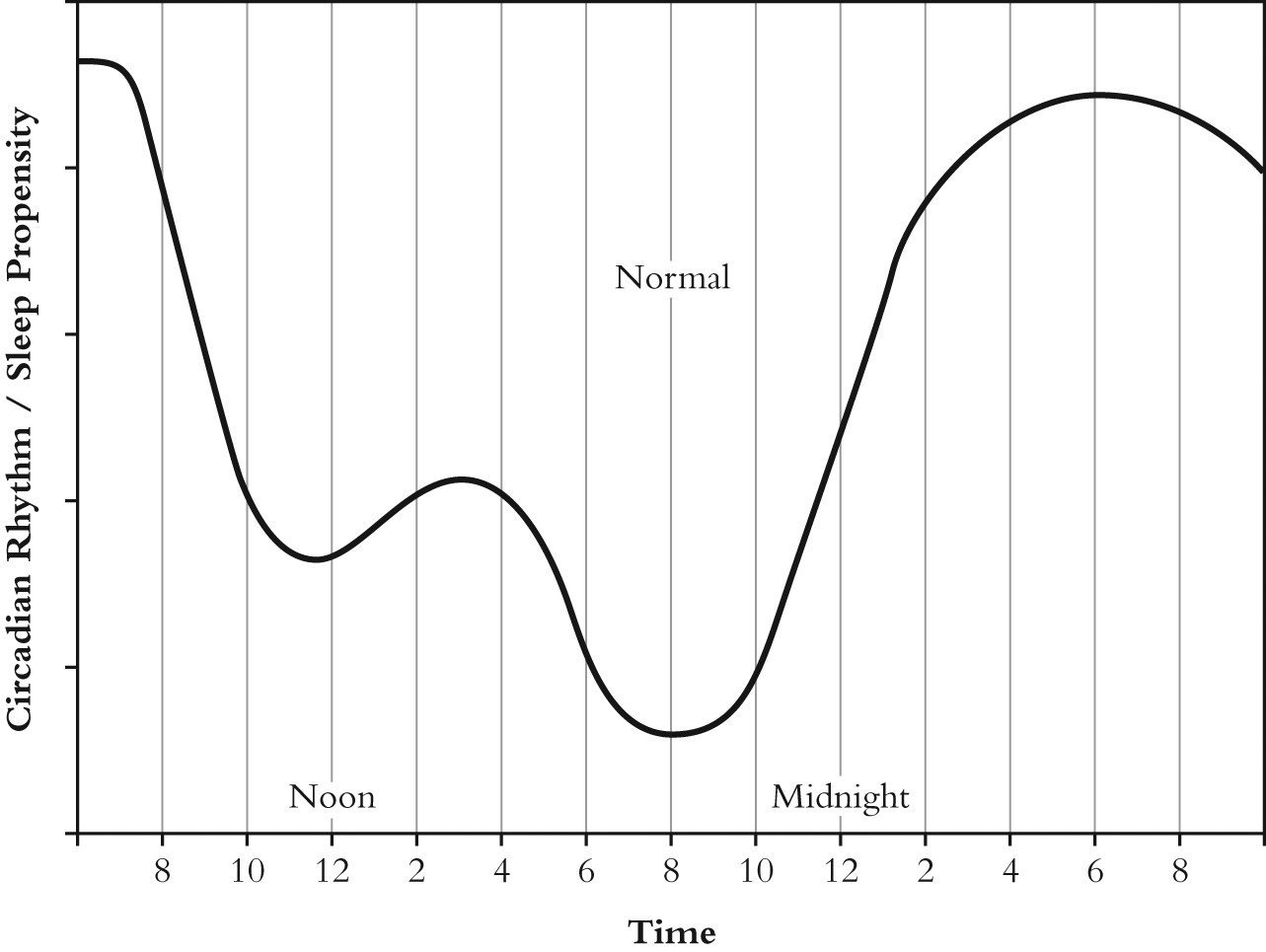
Instead, we could read that insomniac’s little book — and it is a little book — because it tells the truth about why we can’t get to sleep and provides a method, called the Transition Trek, for getting us all the way to Slumberland. Not only that, it tells us how to fix our sleep propensity curve so that we radically improve our inclination to go to sleep and possibly even cure our insomnia. Without redecorating the bedroom. I do like clocks.
The book is called, In Pursuit of Sleep: The Origins of Insomnia and What to Do About It. It is free on this website’s homepage and on iBooks and B&N. Costs 0.99 for the digital on Amazon and $7.99 for the paperback. Click here to buy it online.